
So often patients describe their pain as “sciatica”, too often doctors agree and diagnose their pain as “piriformis syndrome”. But the gluteal region is more complicated that pointing to a spot on your buttock and a diagnosis is made. There are numerous reasons for a pain in your gluteal region. Deep Gluteal Pain Syndrome (DGPS) is an underdiagnosed condition characterized by pain and/or numbness in the buttock area, hip or posterior thigh, and/or radicular/referred pain due to a non-disc related sciatic-nerve entrapment in the sub-gluteal space. To properly diagnose gluteal pathology, a system of orthopedic tests, imaging (advanced and traditional), range of motion testing, and a comprehensive history must be employed before a plan of action may be taken to address the specific condition.
The Anatomy
Before you can diagnosis your pain, you need to know what you’re looking at. The Deep gluteal space borders are:
- Posterior: gluteus maximus muscle
- Anterior: the posterior border of the femoral neck
- Lateral: linea aspera and the lateral fusion of the middle and deep gluteal aponeurosis layers reaching the tensor fascia latae muscle (iliotibial tract)
- Medial: sacrotuberous and falciform ligaments
- Inferior: hamstring Insertion
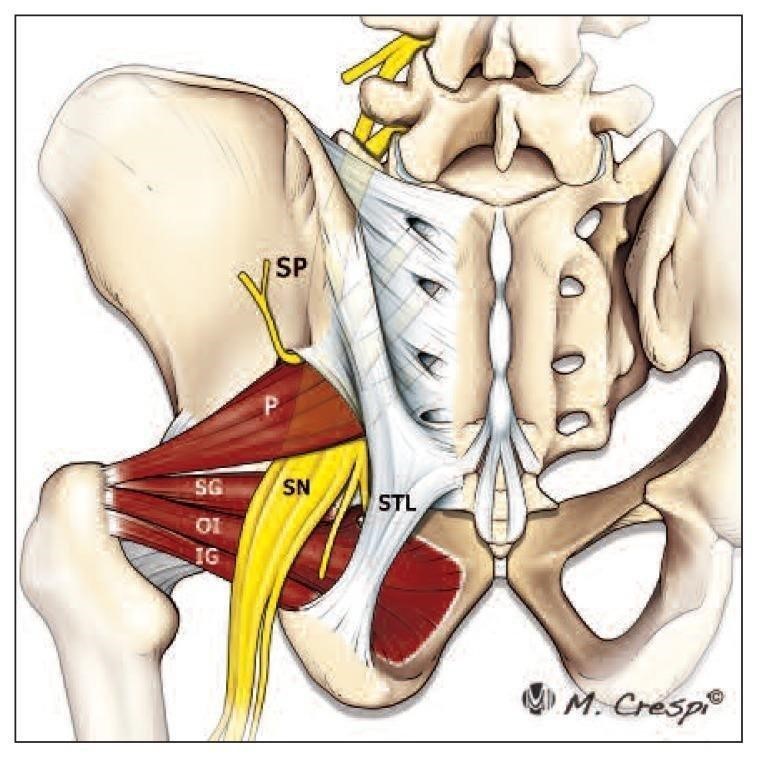
The Contents
- superior and inferior gluteal nerves
- ischium (bone)
- sacrotuberous/ sacrospinous ligaments (STL)
- sciatic nerve (SN)
- piriformis muscle (P)
- obturator internus/externus muscles (OI)
- superior & inferior gemelli muscles (SG, IG)
- quadratus femoris muscle
- hamstring muscles
The Sciatic Nerve
The Sciatic nerve is the largest and longest nerve in
the human body. It originates in the lumbar and sacral
spine with branches of the L4, L5, S1, S2 and S3 nerve roots. These nerve roots unite to what we refer to as the sciatic nerve on top of the Piriformis muscle (in front). From there, the nerve travels posterior (on top) to the obturators, Gemelli and quadratus femoris muscles. It passes between the ischial tuberosity (sit bone) and the greater trochanter of the femur, closer to the posterior capsule of the hip. Once the sciatic nerve exits the gluteal region it enters the posterior thigh/leg where is travels in the middle of the thigh, past the knee and into the bottom of the foot. As there are a lot of “players” in the gluteal region, there are many causes for a potential sciatic nerve entrapment not related to the piriformis muscle.
The Reasons for Pain
There are multiple causes for a DGPS. Specific entrapments, bony deformation/ displacement and injury are the most common.
1. Fibrous Bands
Fibrous Band entrapments are a new concept to anatomist and physiatrists. Typically, the sciatic nerve is able to stretch and glide to accommodate the strain and/ or compression associated with joint movement. But, when bands form over the sciatic nerve, restriction of the nerve during hip and knee movement increases the potential for sciatic neuropathy. Location of the bands, as well as the type/ directional formation may result in various presentations of sciatic pain.
2.Piriformis Syndrome
Piriformis syndrome can be classified as a subgroup of DGPS, but not all DGPSs are piriformis syndrome. Potential causes of piriformis pathology are:
- Asymmetrical hypertrophy (growth) of the piriformis muscle-the piriformis muscle grows too large (hypertrophy) and/or not symmetrical (one area gets bigger than the rest)
- Dynamic sciatic nerve entrapment-with motion, the sciatic nerve is entrapped (crushed) by the piriformis muscle
- Anatomical variations of the sciatic nerve-it is possible, and well documented that the normal course of the sciatic nerve is to pass under the piriformis muscle and posterior to the caudal rotators, but what happens when this isn’t the case? The sciatic nerve gets entrapped. Here are the most common variations of the sciatic nerve entering the DGS.
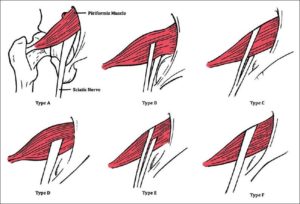
- Type A- Normal, the sciatic nerve passes under the piriformis muscle.
- Type B- The sciatic nerve has two heads. The superior head pierces the piriformis muscle and the inferior head passes underneath, joining with the superior head below the piriformis.
- Type C- The sciatic nerve has two heads. The superior head passes on top of the piriformis muscle, and the inferior head passes below. The nerve essentially surrounds the muscle, joining below the piriformis muscle.
- Type D- An undivided sciatic nerve passes through the piriformis muscle.
- Type E- The sciatic nerve has two heads, one above and one below that pierces the piriformis muscle.
- Type F- An undivided sciatic nerve passes above the piriformis muscle.
3.Gemelli-Obturator Internus Syndrome
Normally not a variant for deep gluteal pain, the sciatic nerve is compressed or entrapped by the obturator internus muscle by passing under the belly of the piriformis, and over the superior gemelli/ obturator internus- causing a scissor like effect. If the piriformis muscle, or the gemelli/obturator are too tight, the sciatic nerve is compressed. Symptoms of this syndrome are traditional sciatic pain precipitated by blunt force trauma or excessive exercise- hiking, jogging or running.
4.Quadratus Femoris and Ischiofemoral Syndrome
Located between the ischial tuberosity (sit bone) and the femur, the ischiofemoral syndrome occurs when fibrous tissue formation builds up and ultimately entraps the sciatic nerve. Symptoms of this entrapment are non-specific pain in the deep gluteal region or ischium, groin or center of the buttocks. These symptoms can last between 2 months and 5 years and usually are not caused by an injury.
Gluteal pain in not easy to diagnosis or treat. In Part 2 of this article we will explore different options/ plans for addressing DGPS, as well as diagnostic testing that can shed a light on a specific diagnosis. It should be noted that while there are several reasons for DGPS, it can be one singular, or multiple reasons for this pain. Remember, the body didn’t come with a manual or play book, sometimes the most obvious reason is the cause, other times pain requires more exploration and critical thinking. If you have an injury issue that needs to be evaluated, please give us a call at 310-534-1900 or email us at info@backtofunction.com.
