
Case Reports
BTF CASE 1
27-Year Old Runner With Left Foot & Knee Pain
A 27-year old female financial advisor reported to BTF with left foot & knee pain with her daily morning runs. She would run up to 6 miles every morning for exercise before work on the treadmill. Unfortunately, the gym in her condo complex, where she was using the treadmill, was closed due to COVID-19 restrictions, so she moved her running outdoors on the streets around her building. This is when she first started having, first the left foot pain, and then the left lateral knee pain.
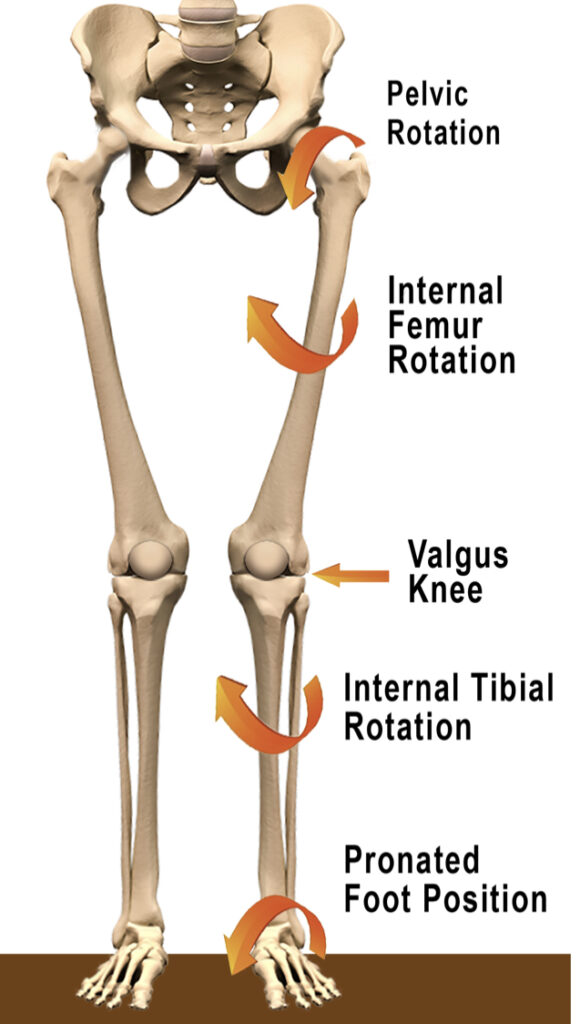
During an initial posture examination at BTF by Dr. Chad Moreau, she demonstrated a moderately pronated left foot and a valgus left knee position. This left foot pronation (dropped arch) puts an increased tensile load on the plantar fascia (bottom of the foot). The left knee valgus (knock-kneed) position puts a compressive load on the outside of the knee and allows the ITB (iliotibial band) to get short/tight on the outside of the left thigh.
During the orthopedic examination & functional screen, she demonstrated:
1) a positive left adduction drop test (modified Ober’s Test)
2) decreased left hip internal rotation at 26 degrees (normal is 45 degrees)
3) decreased right hip external rotation at 27 degrees (normal is 45 degrees)

Inability to get into left hip adduction (see image 1 above) means that she is unable to get her body weight to shift over to the left side efficiently. Add to this lack of left hip adduction is her lack of left hip internal rotation (image 2) and compensatory lack of right hip external rotation (image 3) and we have a situation that creates stress at the left foot and knee.
These postural and functional issues above create tension in the body. Her left lateral plantar fascia, left lateral hip, ITB and thigh and right medial thigh were abnormally tight. She also had a sacral and ilium misalignment that we typically see in someone with low back pain or hip dysfunction.
Treatment over the 4 weeks at 2 visits per week initially focused on myofascial release therapy at BTF to reduce and eliminate the abnormal tension in her left lateral and right medial lower extremities. Chiropractic manipulation of her sacrum and ilium addressed her alignment issues. Shockwave therapy was used on her left foot and lateral thigh in order to break up stubborn fascial adhesions. She was instructed on postural restoration exercises at BTF and then asked to do them every day in order to create a change in her postural and functional asymmetries. For a more detailed look at how we manage knee pain related to postural asymmetries, please check out the article Knee Pain & Posture.
For the first 2 weeks of her recovery, she was asked to just walk for exercise, but she could still do bodyweight exercises like squats and lunges if she didn’t notice them increasing her left knee pain. At week 3, she was asked to do a 1.5-mile run and she had minimal left knee pain at about the 1-mile mark. She was then asked to just walk again for the rest of that week for her morning exercise and to really focus on her repositioning exercises for the rest of the week. At week 4, she tried the 1.5-mile run again and was pain free!
At the week 4 mark the previous functional tests that were problematic were now as follows:
1) a negative left adduction drop test which means that now she functionally has adequate left hip adduction
2) left hip internal rotation at 48 degrees (normal)
3) decreased right hip external rotation at 45 degrees (normal)
Now she will add .5-miles to each successive daily run until she is able to tolerate her longer runs without any left foot or knee pain.
Below is the social media post that she tagged @btfdoc in to thank us for the efficient treatment plan and rehabilitation.
At BTF we absolutely love getting people to FEEL – RECOVER – PERFORM BETTER! If you need help with an injury, please give us a call at 310-534-1900 or email info@backtofunction.com.
BTF CASE 2
47-Year Old Mechanic With Right Lateral Elbow Pain
A 47-year old male exotic auto mechanic reported to BTF with right lateral elbow pain that was exacerbated with upper body exercises in the gym and performing certain tasks involving his right elbow at work. He exercises 4-6 times a week that consists of weight lifting and running. Any movement extending and flexing the elbow as well as supinating and pronating the forearm causes local lateral elbow pain. At work, most tasks include repetitive forceful elbow bending and forearm supination and pronation. He reported to BTF with similar symptoms in 2018 where we were able to successfully treat the condition. However, with the nature of his job and gym training exercises, the elbow pain returned.
During an initial upper extremity evaluation at BTF by Dr. Shelby Kloiber, the patient presented with some postural asymmetry including forward head carriage, increased thoracic kyphosis (increased curve of the mid-back), and increased cubitus carrying angle bilaterally (increased forearm angle away from the body).
During the orthopedic examination and functional screen, he demonstrated:
1. Elbow active range of motion was full but presented pain and stiffness in extension and pronation.
2. positive Cozen’s test presenting sudden pain in the lateral humeral epicondyle
3. positive Mill’s test presenting pain in the lateral humeral epicondyle
4. +2-3TTP: right extensor carpi radialis brevis and longus, extensor digitorum, brachioradialis, and supinator. +1-2 TTP: right lateral head of the triceps and associated distal tendon.
Pain with repetitive one-sided movements, forceful forearm pronation and supination and repetitive vibration has caused an overuse injury, tendinopathy, involving the extensor muscles of the forearm. The most common tendon involved is the extensor carpi radialis brevis. Since the injury is mainly due to his work activity, it leaves us without the option to prescribe rest and avoidance of repetitive activity. Treatment over the 5 weeks including 6 sessions focused on myofascial therapy at BTF to reduce and eliminate the abnormal tension found in the right upper extremity. Therapeutic exercises to increase mobility of the shoulder and elbow due to movement avoidance while in pain, and postural restoration exercises to create a change in his posture and functional asymmetries. Shockwave therapy was used throughout the right upper extremity to break up fascial adhesions, and more directly to induce proper tendon healing of the Extensor Carpi Radialis Brevis through sonic pulsing.
After 6 sessions the results of a re-examination are as follows:
1. Cozen’s and Mill’s Test were negative
2. mild tenderness to palpation of the right proximal extensor carpi radialis brevis and no apparent tenderness of all other muscles palpated
3. active range of motion of the right elbow elicited only minimal stiffness at end range extension and pronation
4. patient is capable of completing tasks at work without pain 90% of the time
Below is the social media post that he tagged @btfdoc and @dr.shelby_dc to thank us for the efficient and effective treatment.

At BTF we absolutely love getting people to FEEL – RECOVER – PERFORM BETTER! If you need help with an injury, please give us a call at 310-534-1900 or email info@backtofunction.com
BTF CASE 3
16-Year Old High School Football Player With a Right Hamstring Tear
A 16-year old male high school football player reported to BTF with right hamstring area pain. He said he was sprinting at football practice and felt a “pulling sensation” in the right hamstring area and felt immediate pain. He said it felt like the hamstring muscle was “balled up” and was “very tight’.
 During an initial posture examination at BTF by Dr. Chad Moreau, he demonstrated a right lateral shift of his pelvis (note how his right arm lies closer to his right hip) and external rotation of his right lower extremity (note how his right foot is turned outward).
During an initial posture examination at BTF by Dr. Chad Moreau, he demonstrated a right lateral shift of his pelvis (note how his right arm lies closer to his right hip) and external rotation of his right lower extremity (note how his right foot is turned outward).

He also demonstrates a significant anterior pelvic tilt (on the lateral view you can also see that his pelvis is rotated to the right).
During the orthopedic examination & functional screen, he demonstrated:
1) positive bilateral adduction drop test (modified Ober’s Test)
2) decreased left hip internal rotation at 23 degrees (normal is 45 degrees)
3) decreased right hip external rotation at 21 degrees (normal is 45 degrees)
Inability to get into left hip adduction (see image 1 above) means that he is unable to get his body weight to shift over to the left side efficiently. Add to this lack of left hip adduction is his lack of left hip internal rotation (image 2) and compensatory lack of right hip external rotation (image 3) and we have a situation that leads to increased work load for the right hip musculature (hamstrings and adductors).
These postural and functional issues above create tension in the body. His right hamstrings and adductors were abnormally tight. He also had a sacral and ilium misalignment that we typically see in someone with low back pain or hip dysfunction.
Treatment over the 2 weeks at 2 visits per week initially focused on myofascial release therapy at BTF to reduce and eliminate the abnormal tension in his right hamstrings and adductors. This breaks up adhesions that form in the fascial layers and increases the blood supply to the injured tissue to stimulate the healing response.
Chiropractic manipulation of his sacrum and ilium addressed his alignment issues.
Shockwave therapy was used on his right hamstrings in order to break up fascial adhesions and improve blood flow to the area which brings vital healing nutrients into the injured tissue.
Compression – Using compression of the injured area in the form of bands (also called Voodoo bands because of their “magic” healing properties). Compression bands are helpful in improving blood flow to the area immediately after the bands are removed. The athlete repeats all the exercises he did with the band, without, after removal.
He was instructed on postural restoration exercises at BTF and then asked to do them every day in order to create a change in his postural and functional asymmetries. The focus on the repositioning exercises was to facilitate the left hamstrings, adductors and abdominal muscles and right hip flexors in order to encourage left hip internal rotation and right hip external rotation while unloading the right hamstrings.
For the first 2 weeks of his recovery, he was asked avoid sprinting and aggressive lower body strength training, but he could still do core and upper body strength training and bodyweight exercises like squats and lunges if he didn’t notice them increasing the right hamstring area pain.
At the week 3 mark the previous functional tests that were problematic were now as follows:
1) a negative left adduction drop test which means that now he functionally has adequate left hip adduction
2) left hip internal rotation at 45 degrees (normal)
3) decreased right hip external rotation at 45 degrees (normal)
Now he will add return to sprinting and more aggressive lower body strength training exercises.
At BTF we absolutely love getting people to FEEL – RECOVER – PERFORM BETTER! If you need help with an injury, please give us a call at 310-534-1900 or email info@backtofunction.com.