
If you are unsure of whether or not you have sacroiliac (SI) joint instability (SIJI), please read the previous article entitled Do You Have SI Joint Pain?. As a chiropractor, I start to consider SIJI when I have a patient who gets relief from adjusting, but never “holds” the adjustment. Another consideration for SIJI is a patient who gets relief and feels better with adjusting, but then trivial trauma, a sudden twist or sitting too long, throws the SI joint area off again, and they return with a recurrence of their low back, buttock and/or leg pain. Sometimes these patients will have generalized ligament  laxity. Can they pull their thumb back towards their forearm? Can they easily hyperextend their elbows or knees? Patient’s with generalized ligament laxity (also called hypermobility) are sometimes very difficult to help. In my experience, it is much easier to get a joint moving more than to make it move less. Regardless, for SIJI at Back to Function, we have adopted a strategy from the Postural Restoration Institute that incorporates key muscle activation creating compressive forces across the unstable SI joint that aids in stability.
laxity. Can they pull their thumb back towards their forearm? Can they easily hyperextend their elbows or knees? Patient’s with generalized ligament laxity (also called hypermobility) are sometimes very difficult to help. In my experience, it is much easier to get a joint moving more than to make it move less. Regardless, for SIJI at Back to Function, we have adopted a strategy from the Postural Restoration Institute that incorporates key muscle activation creating compressive forces across the unstable SI joint that aids in stability.
 Forces that are perpendicular to the joint surface have the most optimal angle of force to contribute to SIJ stability. Externally this can be achieved by wearing an SI Joint Belt. This is a good short term strategy to help decrease the pain associated with SIJI, but a long term strategy needs to be implemented as wearing an SI joint belt everyday is impractical.
Forces that are perpendicular to the joint surface have the most optimal angle of force to contribute to SIJ stability. Externally this can be achieved by wearing an SI Joint Belt. This is a good short term strategy to help decrease the pain associated with SIJI, but a long term strategy needs to be implemented as wearing an SI joint belt everyday is impractical.
There are several different muscles that act to compress and control the SIJs to enhance their stability. These muscles are the gluteus maximus (GM), piriformis, coccygeus, respiratory diaphragm, transverse abdominus (TA) and the internal oblique (IO). It is not enough to simply exercise these muscles, as it isn’t just weakness of these muscles that is causing the SIJI. Postural influences of these muscles can create joint asymmetry in the pelvic girdle and hip joints. The most common postural asymmetry
we see at Back to Function is the Left Anterior Interior Chain pattern (Left AIC) as described by Ron Hruska PT, from the Postural Restoration Institute.
Standing Analysis
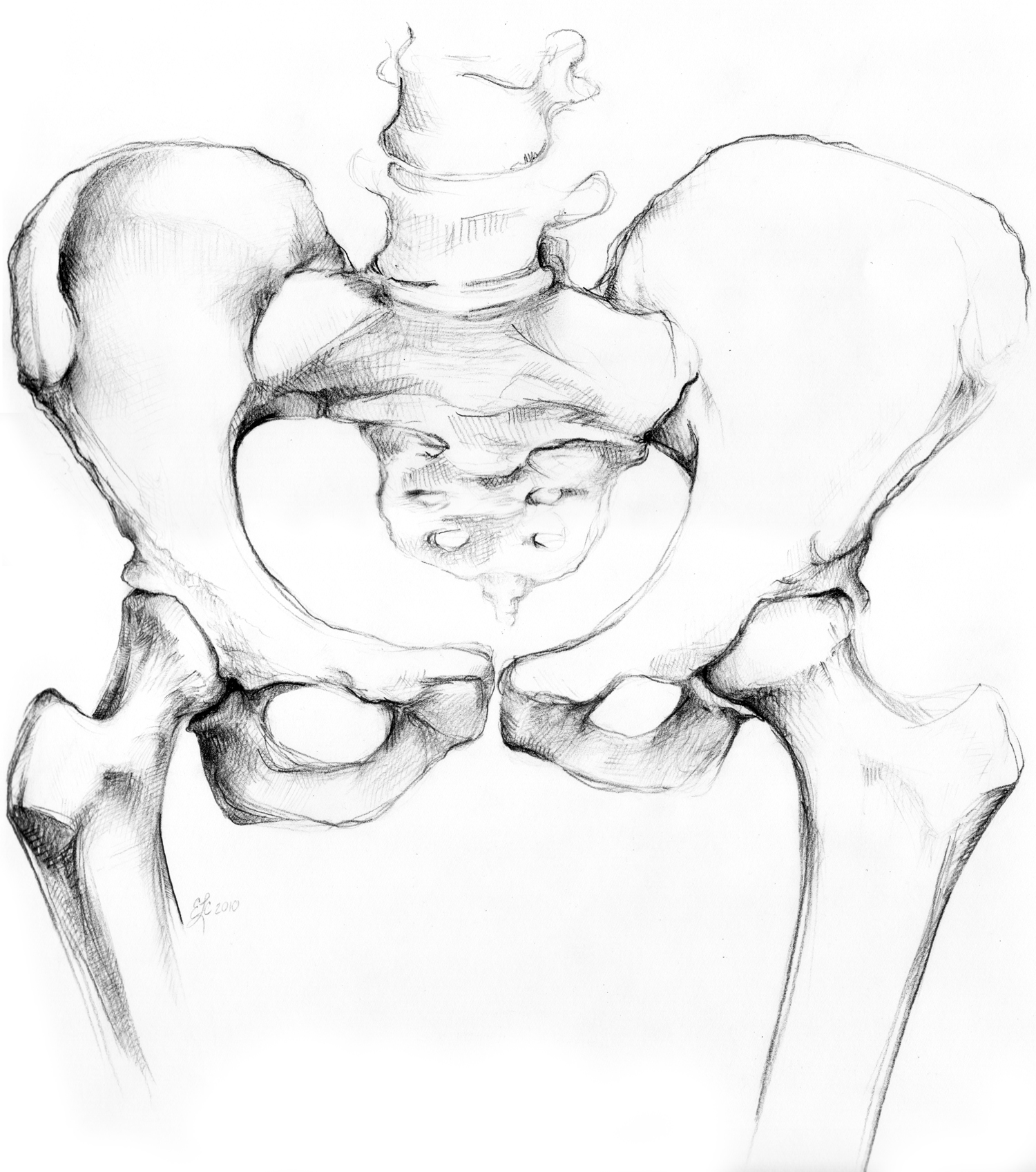
When someone with this pattern stands straight on 2 feet the left side of their pelvis is shifted or twisted forward orienting the spine and pelvis to the right. At the SIJ this causes compre ssive force at the left SIJ and a distractive force at the right SIJ. This position is thought to result from the asymmetrical pull on the spine by the stronger right diaphragm and from the weaker left abdominals. This position is not easily observable with the naked eye but can be assessed by a PRI trained clinician. This pattern can lead to a variety of chronic or insidious injuries and can even effect healing from traumatic injuries. Of interest to us in this article is the effect this pattern has on the SIJs. In standing, this pattern creates a forward rotated position of the left ilium and rotation/torsion of the sacrum to the right (see picture). This would lead to an overuse of the right leg for standing where the center of mass (COM) is shifted to the right. This shift of the COM to the right causes the right hip to adduct and internally rotate. The right groin muscles (adductor magnus) may become hypertonic and short. In order to get more right hip internal rotation, the right ilium would have to attempt forward motion which would create excessive forces across the right SIJ that could eventually lead to right SIJI. The left hip will compensate by abducting and externally rotating. This will cause the left hip external rotators to become overactive. This can cause the left ilium to begin to function more like a left hip joint to increase the available range of motion and this can contribute to left SIJI.
ssive force at the left SIJ and a distractive force at the right SIJ. This position is thought to result from the asymmetrical pull on the spine by the stronger right diaphragm and from the weaker left abdominals. This position is not easily observable with the naked eye but can be assessed by a PRI trained clinician. This pattern can lead to a variety of chronic or insidious injuries and can even effect healing from traumatic injuries. Of interest to us in this article is the effect this pattern has on the SIJs. In standing, this pattern creates a forward rotated position of the left ilium and rotation/torsion of the sacrum to the right (see picture). This would lead to an overuse of the right leg for standing where the center of mass (COM) is shifted to the right. This shift of the COM to the right causes the right hip to adduct and internally rotate. The right groin muscles (adductor magnus) may become hypertonic and short. In order to get more right hip internal rotation, the right ilium would have to attempt forward motion which would create excessive forces across the right SIJ that could eventually lead to right SIJI. The left hip will compensate by abducting and externally rotating. This will cause the left hip external rotators to become overactive. This can cause the left ilium to begin to function more like a left hip joint to increase the available range of motion and this can contribute to left SIJI.
Walking Analysis
When you walk your pelvis and hips are meant to move, shifting back and forth to allow your center of mass to fully balance over the single stance leg. When your right leg is on the ground (stance leg) it is normal for your left half of the pelvis to rotate forward a little. However, in a Left AIC pattern the left pelvis is “stuck” in this forward rotated position and cannot move back adequately to allow the right side to rotate forward. The body will respond with a variety of compensations on both the left and right sides of the body in which some muscle groups will be overused and other muscles will be inhibited. This can contribute to SIJI.
 A pattern that may overlay a Left AIC is called a Posterior Exterior Chain (PEC) pattern. This pattern is characterized by a bilateral anterior pelvic tilt and excessive lumbar lordosis as a result of hyperactivity of muscles in the back. These patients typically struggle to touch their toes or do a full squat. For a thorough evaluation related to SI joint issues, please call us at 310-534-1900 or email info@backtofunction.com.
A pattern that may overlay a Left AIC is called a Posterior Exterior Chain (PEC) pattern. This pattern is characterized by a bilateral anterior pelvic tilt and excessive lumbar lordosis as a result of hyperactivity of muscles in the back. These patients typically struggle to touch their toes or do a full squat. For a thorough evaluation related to SI joint issues, please call us at 310-534-1900 or email info@backtofunction.com.
Part 3 of this article will discuss the management of postural patterns that create SI joint pain.
References:
- http://www.dynamicchiropractic.com/mpacms/dc/article.php?id=51392
- http://www.sarahpetrich.com/uploads/2/6/0/4/26041402/understanding_the_l_aic_pattern.pdf
- Boyle, Kyndall. Conservative Management for Patients with Sacroiliac Joint Dysfunction. www.intechopen.com
